
‘Trauma’ has rapidly become a buzzword in the healthcare sector and the public domain gaining plenty of airtime along with recommendations and different techniques on how to help resolve it. In the wider public domain I believe trauma is still predominantly seen and related to Post Traumatic Stress Disorder (PTSD), or a single event that disrupts an individual’s normal functioning. Even within the trauma sphere, there are also quite a number of different categories to describe where or how the disruption occurred. For me trauma is an important slice in the continuum of nervous system dysregulation, yet it is not always linked to the rapid rise in mental health issues in the general population. For me the state of the nervous system is the highest order, under which both ‘trauma’ and mental health are subsections. So from that perspective I prefer to instead look above any diagnosis, to ‘touch and feel’ what is the state of the nervous system and its regulation or not in my clients as a basis to work from.
As human beings, the nervous system is the mechanism by which we interact with everything around us, from nature and all it encompasses, its sounds, sights and smells to all the other life forms within it. Perhaps one of the most challenging elements in life for our nervous systems are interactions with other human beings. Through our very permeable and vulnerable early years (conception to age two) we absorb into the fabric of our being a felt sense or marker of our safety in the world via the relationship with our prime carer. This psychological theory was known as the Attachment Theory which was borne out of the research of John Bowlby and his assistant Mary Salter-Ainsworth, who further refined the model through her own work. It has become a key concept often referenced in trauma research and understanding. This ‘felt’ sense of safety continues to be refined and nurtured through clear and consistent boundaries (hopefully through conscious parenting) until we have it set in place around the age seven according to teachings of Rudolph Steiner. We are now ready to go out and ‘explore’ the world from a place of deep understanding of what safety is for us. This we carry forward through our entire life as the basis to all relationships to everything outside of us.
A healthy individual who innately feels ‘safe’ in the world has developed a strong and deep sense of how to self-regulate and find their way back from triggering events in life, through self-care, the support of trusted family, friends, their community and professional support.
Then there are those people for whom the world, right from their early years is inherently ‘unsafe’, and who over time and the subsequent adrenal exhaustion associated with that state, lack the resilience or capability to self-regulate and move back into a place of safety. It was never embodied in their formative years. They very often have a very ‘porous’ boundary and deeply feel all the energies around them and in this continual state, contraction starts to have significant impacts on both their organ functioning and structure. We are perhaps all on a continuum somewhere between these two points, yet some have developed a deeper consciousness around their patterning and have learnt strategies, support and self-care practices to keep them in a place of equilibrium. We have ‘lapses’ where we touch into our deep patterning but we are conscious of it and know we have the resources to move out of it. In a way it becomes part of our growth edge. Others remain unconscious of their patterning or ‘drivers’ in life and although they can work hard at ‘coping’ in the world, often have ‘relapses’ where they are thrown back into their deep fear of the world without the self-awareness or support to easily move out of it; they are back at the beginning.
A fundamental understanding in our work as therapists, is that inbuilt within all human beings is a deep knowing in our unconscious being of what ‘safety’ feels like, irregardless of our early childhood years and the subsequent patterns laid down. As such I believe our most important role as shiatsu therapists is to always be seeking to connect with that deep ‘inner knowing’ of safety within our clients as the foundation to start and continue any ongoing therapeutic relationship. Only when we can strengthen that safety through consistency and trust can we support that person in the possibility of change.
My Journey
Although there is a huge amount of information out there on the psychological and somatic approaches to both understanding and dealing with persons presenting with ‘trauma’, in my early days of enquiry, I found very little meaningful discourse in the bodywork realm about how to actually connect and work with the body with people presenting with a background of trauma. Pat Ogden, one of the leading researchers in the field of trauma, states “you just can’t talk your way out of it” and that was my impetus to bring a deeper consciousness to learning and exploring those questions in clinical practice.
What coincided with this, and borne out by a move to Central Victoria, was the need to get a ‘job’ to generate income while I set up a new shiatsu clinic and my partner was unable to work. That for me was working in the disability sector with people on the high-needs end of the spectrum. They have been amongst the best ‘teachers’ I have had and they have also provided me with an opportunity to work with and observe people in an extreme state of nervous system dysregulation, yet with no consciousness, no language nor physical ability to resolve or move back along a continuum to self regulation; they are perpetually frozen.
The rise of Western Culture
In relation to the majority of the human beings that we describe as ‘normal’, we now live in a culture that has evolved into one with widespread accessibility and use of technology and the ‘switched on’ or fight-flight state has extended well beyond the point where we should naturally switch off the yang or doing part of our day and into the yin nurturing part represented by the Kidney time on the Chinese clock from 5pm-7pm. That, coinciding with a 24/7 culture, an increase in shift work and irregular work hours, the time for inner restoration has been dramatically diminished as we either work later into the evening or immerse in ‘device’ time in an attempt to ‘switch off’. Alongside that has been the rise in illicit and licit drugs, caffeine drinks, sugar, and a processed fuelled food culture to boost what we have not cultivated by a consciously healthy lifestyle.
In reality, we are highly unlikely to die nowadays going about our daily life, so the nervous system fight-flight state has become normalised; we sort of know it’s not right but it’s just how things are! So there is a conflict within the system; the visceral response is to activate the nervous system to resolve the ‘danger’, yet the brain (and culture) says it’s ok; ‘there is no danger’, we are not under threat and this is ‘normal’. This creates a perpetual internal conflict, and in order to participate and thrive in our current western way of being, accepting this as the norm and going with the culturally ‘acceptable’ flow is less challenging, albeit unsustainable. ‘Suck it up’ has been a mantra for decades. The human body, in my mind, is showing a consistent reflection of this way of being in the body; there is a conflict between shutting off and staying switched on. The body wants to curl up into a ball, yet the cultural need to conform and be part of the ‘group’ disconnects us from what the body is saying. In my observation a lot of clients have moved beyond the fight-flight into a ‘freeze’ response which is often locked in a specific part or parts of their body.
The Bodily Response
In relation to trauma, renowned author Gabor Mate says:
“Trauma is not what happens to you, but what happens inside of you because of what happened”
Having worked in clinical practice since the mid-1990’s, within the disability sector for 10 years and with numerous people with PTSD, Complex Post Traumatic Stress Disorder (C-PTSD), and a whole array of mental health ‘disorders’, I have come to realise that although the ‘what happened to them’ is quite different, the way the body responds, or the ‘what happens inside of them’ manifests consistently in some key areas of the body. They are in my mind the same in the case of PTSD/C-PTSD as they are for people in a perpetual and ‘normalised’ state of fight-flight or freeze.
In saying that, everyone is a unique being and comes with their own history and patterning and so it then becomes crucial in how we engage and work with different people; we need to find and work out the way forward together in a mutually responsible therapeutic relationship. There is no one size fits all and a key part of the movement back towards self-regulation is supporting them regaining power and agency over both their body and life. Good treatment offers an opportunity to practice that in the microcosm of a safe environment.
Central to a visceral ‘fear’ response is a contraction of the psoas; an unconscious muscle that Liz Koch suggests is perhaps more an organ of the nervous system than a muscle; the fight-flight muscle if you like. As muscles operate in groups and across areas, so does the influence of the psoas. Its origin is both the body and the transverse processes of the lumbar vertebrae and its attachment is on the medial aspect of the femur. When it contracts, it is essentially seeking to pull both the upper and lower body together into a foetal position.
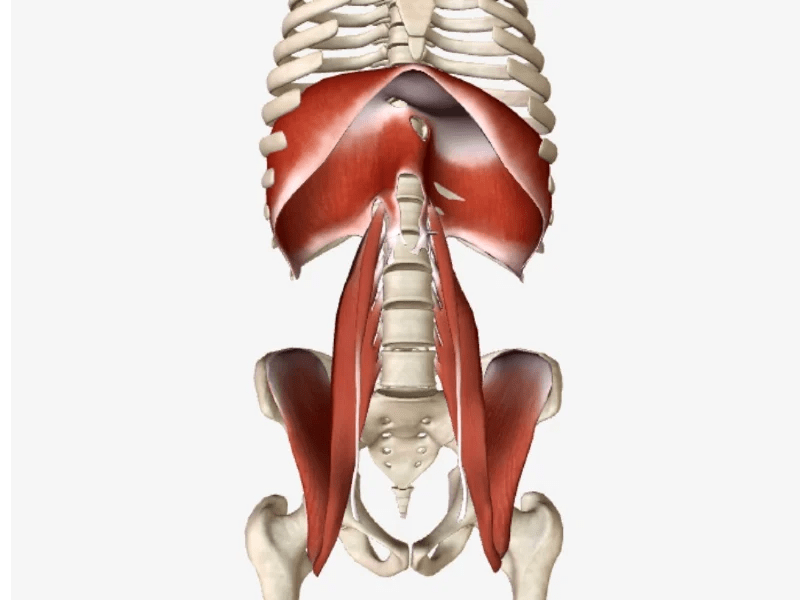
Also attached to the body of L1- L3 are the crue of the diaphragm, or the two tendons, like strings of a kite of the jellyfish-like muscle that sits between the abdomen and the bottom of the lungs. Significantly, the diaphragm has three large openings (and several smaller ones) or ‘holes’ through it:
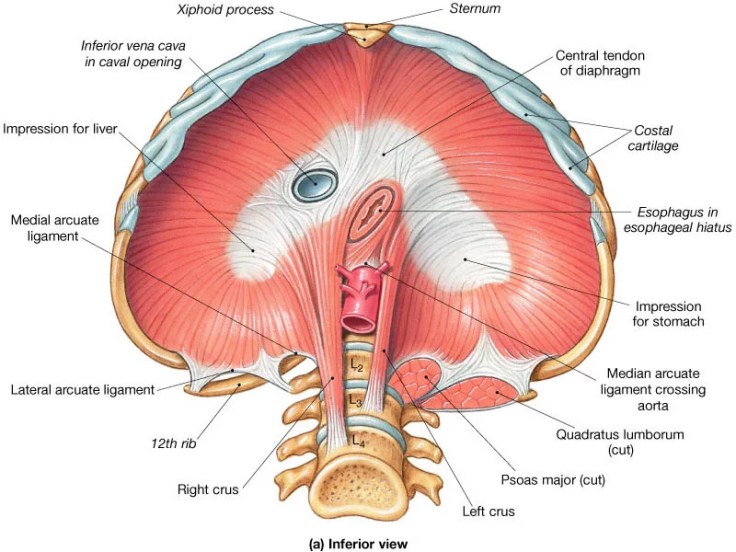
- The Oesophageal opening (oesophageal hiatus) through which the oesophagus, the right and left vagus nerve, and the left gastric artery and vein pass;
- The Aortic opening (aortic hiatus) through which the aorta, thoracic duct, and the azygous vein pass;
- The Caval opening (cavus hiatus) through which the inferior vena cava and parts of the phrenic nerve travel.
- In addition there are also several smaller openings that allow smaller nerves and blood vessels to pass through.
So the tension of contraction present in the lumbar vertebra due to the psoas pulling it downwards, inhibits the free movement of the diaphragm. This not only impacts the healthy functioning of breathing, but also constricts to some degree all those key elements that pass through the openings. In addition, as it is pulled down it also restricts the space of all the organs contained within the abdominal cavity, which will affect their healthy movement and functioning. They need space to ‘breath and move’ to function normally which is provided by the rhythmic movement of the diaphragm acting like a pump that facilitates and supports those movements.
The other key muscle connecting into this area is the trapezius, whose origin points are the base of the skull and the spinous processes of C7 and T1-T12. Its insertion points are the lateral third of the clavicle, the acromion process and the spine of the scapula and its sphere of influence covers the thoracic spine, the shoulders and the back and sides of the neck.
Both the Trapezius and the Sternocleidomastoideus (SCM) are only two major ‘long’ muscles in the body innervated by a cranial nerve; cranial nerve XI. The only other muscles governed by cranial nerves are the muscles of the head and face and these are the areas of our body that are integral in determining our degree of ‘social engagement’ or safety in the world; we first need to be able to look and hear around us to others as to whether we are in danger or not.
Stanley Rosenberg writes that “the CN (cranial nerves) V, VII, IX, X, XI all need to function properly if we are to be socially engaged” He goes on to say that “in order to function properly, these cranial nerves need an adequate blood supply” and that “rotation of the cervical vertebra can reduce the blood supply to the brainstem, resulting in an dysfunction in these cranial nerves”
So from that we can possibly conclude that the perpetual fight-flight state and its subsequent contractions within the body create a vicious circle; the tension up into the trapezius and its attachment points are likely to pull on the cervical vertebrae thereby possibly restricting the blood supply to the brain, which then impairs our ability to be socially engaged or safe. That tension will also impact the facial muscles and the SCM further perpetuating the dysregulated state. Burnout or breakdown, be it mentally or physically has become a feature of our evolving western life. This adrenal fatigue is the precursor to a whole myriad of chronic health issues.
Integral from a structural and emotional perspective is the whole vertebral column and the rib cage. The vertebral column is where all those key muscles attach and the rib cage articulates with the transverse processes and body of the thoracic vertebra. The rib cage both contains and protects all our vital internal organs; the domain in my mind of the Pericardium or Heart Protector as Masunaga named it. For me, that best describes its function which is to protect the Heart. In Zen theory its role is to determine when it is safe to open and when it is not in relation to our interactions with our fellow beings which is very aligned with the function of the nervous system. Its yang pair is the Triple Heater whose role is to adapt to the social and physical environment around us.
So the tension radiating up the vertebral column moves out and around the ribcage to the sternum, further constricting the movement of the Lungs and Heart and creating a solid and armoured upper burner region. It is like the elite soldiers protecting the emperor within, and any battle with it is likely to be lost. Attempting to work forcefully into this region in my mind only serves to further exacerbate the protective functioning. We need instead to come with love, openness and a desire to help and support before we will be ‘allowed in’.
So from what I see to be the ‘centre’ of the visceral nervous system response, the thoracic-lumbar junction, we have the psoas going down, the trapezius going up and the diaphragm wrapping around. If we have a disruption in the normal functioning of our nervous system, be it through being in a state of perpetual fight-flight, a specific traumatic episode or repeated episodes, all these muscles are initially in a state of tension and readiness before eventually unconsciously being pulled inward to the centre as the stressors are unresolved.
The attachment points of these key muscles are a good indicator to the state of the nervous system. How mobile and free is the thoracic-lumbar junction region on the back; is it stiff and held or does it move with freedom? The corresponding area in the abdomen is around the solar plexus or the Heart Protector diagnostic zone in the abdomen; is it soft and pliable or a hard lump, often with a strong pulse that in my mind is because of the constriction in the aortic hiatus? Again, where the trapezius meets the skull; is it soft and malleable or does it feel tight and wirey?
Chronically disabled persons with cerebral palsy are an indicator of an extreme; there is a deep and frozen contraction in the system pulling towards the centre; this affects all the tendons, ligaments and muscles on a physical level. Those in a perpetual state of fight-flight are at the start of the same continuum; tensions radiate out from the core
Around the trapezius/SCM attachments in the neck there will be chronic neck and facial tensions, primarily impacting neck mobility and jaw tensions. Their attachments to the clavicle and the spine of the scapula, coupled with tension in the entire ribcage create tensions in the shoulder girdle with subsequent problems down into the elbow and joint issues in the hands. Breathing will also be restricted in some manner and this mechanism is the prime mover of Ki in the body
Radiating out from the thoracic-lumbar junction will be tension under the ribcage and constriction to all the elements that move through the many openings in the diaphragm. Digestive problems are very common along with sluggish and erratic intestinal movement. Breathing into the abdomen will often be challenging
Radiating out from the psoas attachment and down from the centre there will be pains in and around the whole pelvic girdle, the hamstrings will most often be tight with tensions radiating down the upper leg muscles and tendons into the knees, ankles and feet
So how are we going to work with that in our clinical practice? How can we relax their body and switch off their overactive nervous system?
Before I even think about what I’m going to do, I firstly need to ask how do we build a framework for a relationship that will support them back to a place where they can start self-healing? This is my fundamental framework for treatment.
Foundations of Treatment
Now when we work with any new client, let alone those with any sort of nervous system dysregulation, their system will naturally be in a state of ‘fight-flight’; they are entering into an new relationship so need to have their guard up until it has been determined that it is safe for them to relax and trust. This is a normal and healthy functioning of the nervous system. For anyone with trauma or any long term stress or tension in the system, this will be a process that will evolve over time as opposed to happening in one treatment. For some clients it is years before their body can ‘let go’.
Stephen Porges states “feeling safe is the treatment” and this for me becomes one of the key principles of my practice in treating every client. When one feels safe, the nervous system and body has an innate in-built self-healing mechanism. As therapists, we cannot ‘fix’ anyone; we can only facilitate a space where they can access their own self healing response. I have often shared with clients with complex trauma and safety issues that we are continually creating and strengthening their connection to an embodied or visceral sense as to what safety feels like within their body.
From that perspective, setting the tone and agreement for the therapeutic relationship is vital; it is a framework that acknowledges the way in which the relationship will be conducted. Central to that is another of my key treatment principles and that is ‘they know their body better than I know their body’. As such, they are the ones leading the treatment; my role is to listen, to constantly adjust to both their verbal and non-verbal direction and to keep checking in, both with them and myself, as to whether we are ‘meeting’ at the point they need to be met to feel, and stay feeling safe. This often at the beginning of a treatment relationship is verbal and very often; they need to know from my actions that I am seeking to be the listener, not the leader. My expertise if you like is to know those parts of their body I need to contact and be with and in naming their bodily reactions if I sense them to affirm they are real.
One of the key learnings for me in working with people with high needs disability, who we can view as a cohort all with C-PTSD from birth, is that they need to know at all times where I am and what I’m doing or about to do and this needs to be communicated. Secondly, I need to be really tuned in to what their body, via sound, posture, complexion and body language is telling me in terms of what I’m doing. This is vital to bring into working with anyone, regardless of their state.
So before we even put our hands on our clients body, I believe there are important concepts to understand in order to be able to create a safe space for our clients. Two of those concepts for me are Mirror Neurons and Counterwill.
Mirror Neurons
In the mid-1990’s, scientists identified what later became known as ‘mirror neurons’. This understanding helped explain many previously unexplainable aspects of the mind such as empathy, imitation, synchrony and the development of language. They are what enable us to pick up another person’s movements, their emotional state and well as their intentions. They also start functioning as soon as we are born and are a key factor in our developing relationship with our prime carer, often the mother, validating the earlier work of John Bowlby and Mary Salter-Ainsworth.
When we are in harmony with each other we tend to mirror body language and reflect each other’s energies. Conversely they also make us more vulnerable to ‘negative’ energies around us. Good treatment needs to reactivate the capacity to safely mirror and to be mirrored by others, but also to be able to resist being overwhelmed by others’ negative emotions.
We need to ensure that as practitioners that we are on a journey of exploring our own psychological patterning in order to be able to help our clients resolve theirs. We need to feel centred and connected to who we are; we need to be comfortable in our own ‘skins’ before we can truly hold the safe space for our clients to find and inhabit that within themselves. That is in essence what creates a good therapist; a deep and conscious awareness of who we are in the moment.
Counterwill
Counterwill is defined as a psychological term that means “instinctive resistance to any sense of coercion”. This can be both explicit or implicit. In other words, as soon as clients sense I want them to do something or I am seeking something from them, they will resist, even if it is potentially good for them. Remember, that via the mirror neurons, they will know even on an energetic and thought level.
For me in a treatment, it again needs me to honestly ask, am I seeking something from my client? I may have a deep desire to fix something or do something to fix something or have a desired outcome I want for them. They will most often come in wanting you to fix something.
Can I truly let that all go and focus upon simply meeting them in the place that creates safety? Nowadays I tell them directly I can’t ‘fix’ them. I can only support them to find and ‘fix’ themselves
Creating a sense of personal power and ‘agency’ is central in bringing the nervous system back along the continuum to safety; the only true healer is that which is inherent within each individual.
Client-Practitioner Relationship
A challenge we have in our modern times of seeking to be professionally recognised is how do we find and maintain a deeply authentic presence within all we are told what being ‘professional’ means? The scientific western approach is still based on the concept that the mind and the body are separate, even though it is widely known and understood that this is not the case. I think the concept of being professional is part of the western paradigm that does not take into account the emotional human being within. I’m sure most people will relate to that through some instance or rather in life where they were seen as separate from their illness/problem etc. It has never felt right to me, and it certainly never elicits either a deep trust or safety.
Can you trust someone who is hiding behind a facade? Professionalism has been taken over by the fear of doing something wrong, and out of that fear comes a kind of emotional detachment, not committing to be open and vulnerable operating from the heart. I have long advocated and taught students to be ‘unprofessional’.
Perhaps we could choose to reframe the idea of what it means to be a professional. If we aspire to be truly effective, I believe we need to be authentic and from our heart, to share our own vulnerabilities and challenges in life where appropriate in order to build and demonstrate an empathetic connection that can take trust to a deeper level. People with nervous system dysregulation need help from someone in a regulated state, firstly through co-regulation, in order to help them move along the continuum to self-regulation. We need to continue to work on our own regulation in order to be able to help others co-regulate.
However, integral to that way of being is having very clear and transparent boundaries around the relationship so we can create a safe container for exploration to happen and not create dependence. In other words, be an emotional and authentic human!
Remember, our clients will know where we are at, not necessarily on a conscious level but in their gut and this is the driver of the nervous system response.
Treatment
Once we have defined the parameters of our relationship, how do we take that into the treatment we give? This is our role as the ‘yang’ partner in the relationship
Over the course of my shiatsu journey I have realised that all the training I had done from the time I first started shiatsu that really resonated with me was around developing a safe connection. These are the things I have continued to practice, evolve and deepen through clinical practice and I have circled back to understand now that is what perhaps Masunaga meant when he created his five principles of Zen Shiatsu:
- RELAX; which is self explanatory as that is what we are wanting to mirror!
- PENETRATION NOT PRESSURE; listen and follow your clients cues rather than treating from the head in a predetermined fashion.
- 90 DEGREE PERPENDICULAR PRESSURE; meet your clients directly face to face
- TWO-HANDED CONNECTEDNESS; hold your clients with as many points of connection as possible; like a loving parent with their baby.
- MERIDIAN CONTINUITY; listen and follow.
Connection
Once we understand key elements of what determines safety then the next question is how do we touch? Are we working on a ‘part’ of their body with an objective in our mind to fix a problem? Do we stretch something out because we ‘know’ it will help them? Do we move without consciousness to get to the next part we want to ‘work’ upon?
John Bowlby[5] in his Attachment Theory and Mary Salter-Ainsworth for her collaboration and continued development of that theory, state that in order for a child to be ‘safely’ attached to their prime carer, three things are seen as crucial; loving touch, emotional availability and being emotional attuned.
Loving touch to me is touch without expectation; we touch because we both care and are seeking to understand through feeling without judgement.
Emotional availability is not shying away from what is there, but embracing wherever someone is at with openness and curiosity to understand their deep needs below the feelings. It is being open and willing to deeply listen with empathy.
Emotional attunement is an instinctive knowing when something, be it mental, emotional or physical is present in another and addressing that to enable them an opportunity to express or shift what is there.
Movement
Once we have made contact through a loving touch how do we maintain that throughout our session?
In my mind chaotic and random is unsafe, whereas predictable, smooth and flowing is safe.
Do we move around the body with a smooth predictable flow from our centre and in our heart? Or do we jump from one place to another losing physical contact as we do. I have always seen and felt this on a deep level to be abandonment; the client has ‘lost’ us and doesn’t know where we are. This activates a startle reflex on a deep level when we show up somewhere else.
For me the transitions around the body are a crucial element in facilitating a sense of safety in our receiver that is often overlooked and given little attention in the need to get to the next place to work upon. All movements are full of ‘information’ about the state of the body and so it is important not to ‘switch off’, but rather to take the time to deeply listen to what their body is saying at all times. In order to do this we need to learn how to move from a place that is relaxed, open and from the hara and heart so it becomes part of the beautiful dance of deep connection and ‘meeting’ we are continually seeking to inhabit.
This is often not taught or its importance reinforced due to the lack of time within the modern diploma structure. For me it is one of the fundamental foundations and has been one of the cornerstones of my teaching.
Perhaps now there is nothing more to do to effect a change in their nervous system, yet the mind has come with an acute awareness of the areas of tension in the system and so we need to address those in order to leave them with a feeling their needs have been met.
How we take those principles and understanding into clinical practice and actually work with the bodily nervous system response is beyond explaining in an understandable way via the written word so check out my post-graduate training program which will cover the synthesis of my shiatsu journey to date.
